I must admit I’m not entirely sure which techniques Osteopaths use, but as far as I know they combine things from Physiotherapy, Chiropractic-therapy and massage therapy. I would expect manipulations, various mobilizations/joint play (Mulligan, Kaltenborn, Maitland), McKenzie, MFR (myofascialrelease), triggerpoint, soft tissue releases, massages and the like. They are specialized in manual therapy, but they do include nutrition and exercise as well. Of which quality I couldn’t say, but I think using a multifactorial approach to care is smart if done right.
Regarding the literature there’s a lot to unpack. It’s important to consider the scientific and methodological limitations when it comes to high quality evidence for manual therapy. It’s hard to standardize reps, force and application. Inter-reliability is low as it's in many ways an individualised skill. Another important qualifier is choosing the right manual tool for the right underlying pathology. That takes diagnostic ability and experience, which is unfortunately lacking in many (manual) professions. Lastly patient response varies with different tools.
With that in mind let’s take a look at 1) Manipulations, which I use sparringly, but are very prevalent, and 2) The Mulligan Method, which I use more often. While I believe that the rest have merit, I won’t go into them here.
Manipulation
Discarding original concepts of quackery like “curing all diseases” and “putting misaligned joints back into place”, manipulation does seem to have an immediate pain relief and muscle-tendon relaxation property in most cases. A few studies have showed reduced short-latency stretch reflexivity after spinal manipulations with an audible “pop” (
1,
2) and others reduced tone in paraspinal muscles on EMG readings following treatment (
3,
4,
5). However increased tone has also been noted (
5). A meta-analysis from 2012 showed a mean increase in pain tolerance when exposed to various pain inducing effects after spinal manipulations (
6). Other studies have shown an increase in heart rate variability (HRV), and improved vagusnerve stimulation, all markers for parasympathetic activity (
7,
8), although this change could not be shown to correlate with pain decrease in a single study (
8).
The parasympathetic system is the so called “rest and digest” part of the autonomic nervous system. This might be a plausible hypothesis as a contributing factor to the relaxing feeling accompanied by a “pop” or “crack”.
A systemic review in Spine from 2004 discussing the efficacy of spinal manipulations and mobilization on low back pain and neck pain, concluded that both could be recommended, yet that more evidence was needed (
10). Moving on, two meta-analysis specificly looking at manipulations and outcomes on acute low back pain and chronic low back pain, the latest Cochrane reviews from 2011 and 2012 respectively, concluded that spinal manipulations showed no better outcome compared to other modalities (
11,
12). This was including sham and intert interventions. Others have discussed the difficulties in finding statistical significant differences in something as multi-dimensional as low back pain (
13), and it’s important to consider that the heterogeneity of groups and patients makes it difficult to discern outcomes.
There seems to be no high-quality evidence to suggest spinal manipulations as superior compared to other treatments, especially long term, but there is low-moderate evidence to show that is has a positive effect on pain and function.
A new Spine meta-analysis from this year, 2018, came to that same conclusion (39).
In regards to safety, more aggressive reviews have suggested that spinal manipulations, especially cervical ones, have a high incidence of adverse side effects, including high risk ones (
14), however later prospective studies and reviews suggest a low incidence rate of severe adverse effects. Mild side effects like headaches, dizzyness and numbness seem relatively common (
15,
16,
17).
Mulligan
Mulligan is based on the anatomical structure of joints and their joint play, or arthrokinematics, including glides and rolls. While others like Kaltenborn and Maitland (
18,
19) have previously used passive joint play in an attempt to improve ROM, function and pain, Mulligan introduces active movement from the patient concurrently. In that way, the mulligan method takes into account both the arthrokinematics and the osteokinematics of the joint.
Mulligan uses three primary tools. SNAGS (Sustained Natural Apophyseal Glides) and NAGS (Natural Apophyseal Glides) for the (cervical) spine, with the main focus being MWM (Movement With Mobilization) which targets the extremities.
An early meta-analysis from 2009 concluded that there was moderate evidence to support the efficacy of MWM on the extremities (
20), however a more thorough meta-analysis from 2011, made at the Physical Therapy World Congress, concluded that further evidence was needed. They did find moderate evidence to support positive outcomes on ankle sprains, cervical headaches and tennis elbows (
21).
Many RCT studies have been conducted since then and shown improvements in ROM, strength, stability, pain and function in patients with various musculoskeletal pathologies of the ankles (
22,
23), shoulders (
24,
25), hips (
26), trunk (
27), lower back (
28) and neck (
29,
30,
31,
32). This is compared to control and sham groups, and in some cases other manual modalities (
25,
27,
31,
32). There’s also evidence to support MWM with exercise being more beneficial than exercise alone (
27,
33). Some pilot studies even show improved gait, weight bearing and postural control in stroke victims after ankle MWM (
34,
35).
A study using Maitland and Mulligan did show slightly less pain reduction comparatively for the Mulligan treatment in regards to low back pain, but increased ROM (
36).
The physiology and anatomy of the positive effect outcomes is not yet understood. The translation of joint surfaces could help reduce biomechanical issues in the joint, and therefor improve ROM and pain. Some have hypothesized a neurophysiological component in guiding movement with active muscle tension, as this theoritically could reinforce somasensory feedback, and improve motor patterns. This is not well documented at the current time. There is of course also the array of biopsychosocial factors that should be considered in the outcome of any manual therapy.
I think that manual therapy professions, including Osteopathy, can be very valuable for a variety of reasons. How valuable depends in large on the clinician. As a physio I don't believe they can or should be the only modality, but I'm also not one to suggest that they should be discarded. I actually find that notion quite foolish.
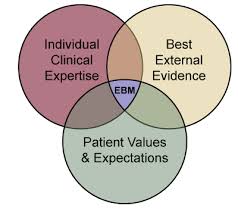
Untill we uncover some of the more intricate physiological mechanisms, if we do, I think this model is a good representation of a lot of the non-specific affects that seem to influence the efficacy of manual therapy:
Notice the upper right corner. The evolution of pain science has becomes a part of practice. The pain matrix with the various factors like cognition and emotion is an expression of the complexities of pain. Call it placebo, call it fear avoidance, or call it an autonomic, hormonal and neurological response that is not quite well understood.
Evidence based practice has been a gamer changer in the world of rehabilitation therapy, and it’s incredibly important. Something we couldn’t and shouldn’t do without. With that said, there are limitations in regards to contextual factors. Everything is calculated in means, and the individual is often drowned out in the stats, which is something you see in the clinical setting often. That is disregarding bad science of course, which there is a lot of too. That’s not a knock. Making a good study is a hard thing to do and biases exists in us all.
Proof is in the pudding. In in my opinion, patient response and clinical outcome is the most important factor in administering rehabilitation, but best practice is still a multifactorial approach.
http://data:image/png;base64,iVBORw0KG
PS: Just a fun little nugget. A study in which healthy subjects improved their pulmonary function as an expression of FEV’s, after manual therapy on the thoratic spine (
37), although another one by a different group of researcher couldn’t replicate the findings (
38). It’s important to note that there were differences in interventions and that the one which couldn’t replicate the findings only had one sessions, versus 3 in the one that could. Safe to say that the validity of this methods would be better examined using patient groups with obstructive lung diseases.
EDIT:
This is gonna stay here temporarily as the thread it was posted in was deleted. 
")